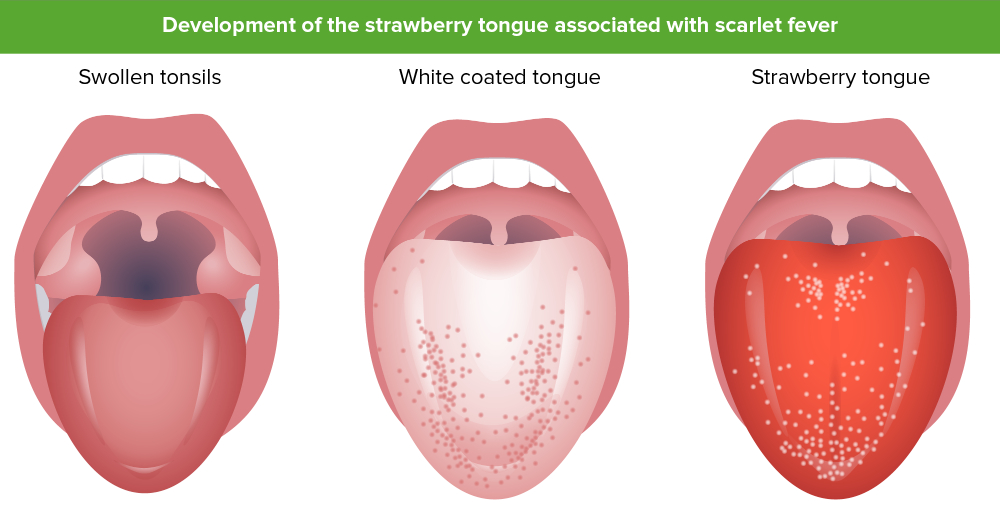
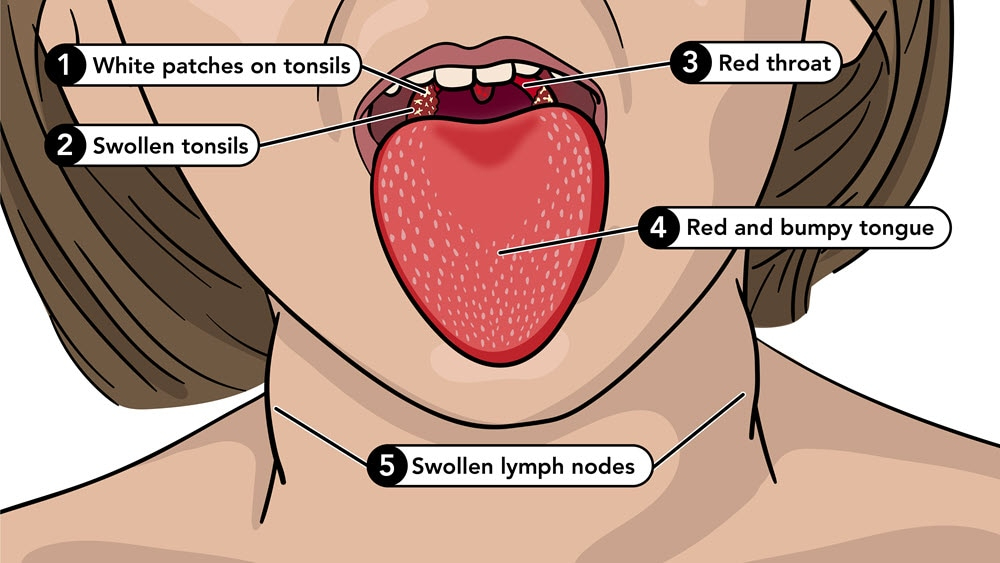
Scarlet fever is an infectious disease primarily affecting children aged 4-8, often resulting from a hypersensitivity to streptococcal erythrogenic toxin. Symptoms include sore throat, fever, and a distinctive red rash. Oral manifestations include “strawberry tongue,” characterized by a white coating and swollen papillae, which later transforms into “raspberry tongue.” Treatment involves penicillin, and oral symptoms typically resolve within 14 days.
Age Group: Affects primarily 4-8 year-olds.
Cause: Linked to streptococcal toxin hypersensitivity.
Symptoms: Includes sore throat, malaise, fever, and rash.
Oral Manifestations: “Strawberry tongue” and “raspberry tongue.”
Treatment: Penicillin is the main medication used.
Recovery: Oral symptoms usually resolve within 14 days.
Rash: Characteristic red rash is a key indicator.
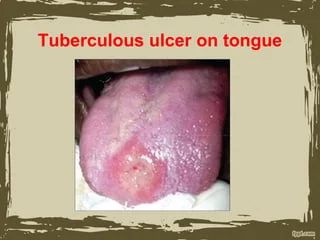
Tuberculosis (TB) is a re-emerging infectious disease primarily caused by Mycobacterium tuberculosis, often affecting immunocompromised individuals, including the elderly. Although TB is rare in Western countries, its incidence is rising due to factors like migration and HIV spread. Oral involvement is uncommon but presents as painful ulcers, are secondary to lung infection through seeding by sputum, typically on the tongue. . Diagnosis can be supported by PCR and histopathology. Treatment requires referral to a chest physician for combination chemotherapy, and in children, lymph node excision may be necessary.
Type of TB: Latent (can't spread and the person doesn't have symptoms), or Active (serious disease and fetal, patient have symptoms and can spread disease)
Re-emerging Disease: TB is increasingly reported, especially in Western nations.
Immunocompromised Risk: Primarily affects the elderly and those with weakened immune systems.
Oral Involvement: Painful, Chronic indurated non-healing ulcers, often on the tongue. Tuberculosis osteomyelitis, Scorfula ( irritated lymph nodes, cervical or submandibular)
Diagnostic Tools: PCR and histopathological analysis
TB Tests: Tuberculin skin test: result observed after 2-3 days (Type IV hypersensitivity reaction), TB blood test: IGRA.
Histopathological Findings: Reveals necrotizing granulomas with Langhans giant cells and epithelioid cells and a Ziehl–Nielsen stain reveals mycobacteria.
Treatment Protocol: Requires referral to a chest physician for combination chemotherapy.
Children’s Treatment: Lymph node excision may be needed in pediatric cases.
Global Impact: One-third of the global population is affected by TB
*^NB: infection control:
1-Addminictrive: written instructions, and staff education about symptoms and symtpoms, having plan to reduce exposure.
2-Environmental: Isolated rooms for suspected or diagnosed patients, HEPA filters
3-Protective: N95 mask for staff and surgical mask for patient.
Patient consideration:
- Latent: non treatment modifications
- Active: Elective:( defer dental treatment and refer to a GP), Urgent: (follow infection control steps *^)
Syphilis is a sexually transmitted disease caused by Treponema pallidum. It progresses through three stages: the primary stage presents a painless ulcer called a chancre, the secondary stage includes a widespread rash and systemic symptoms, and the tertiary stage can lead to severe complications such as gumma formation and central nervous system involvement. Early diagnosis and treatment are crucial to prevent long-term health issues.
Primary Stage: Chancre (a firm, painless ulcerated nodule, Genitalia and anus are the most common sites.
Secondary Stage: cutaneous rash, condylomata and systemic features such as malaise, fever, headache, and weight loss. The oral lesions include sensitive sloughy mucous patches known as snail-track ulcers and condyloma latum.
Serology: Positive tests during the secondary stage.
Tertiary Stage: Is a multisystem disorder causing CNS involvement and vasculitis.Gummas due to perforation of the palate and syphilitic leukoplakia.
Cervical Lymphadenopathy: Swollen lymph nodes that resolve spontaneously.
Transmission: Highly contagious during primary and secondary stages.
Treatment Importance: Early intervention prevents severe outcomes.
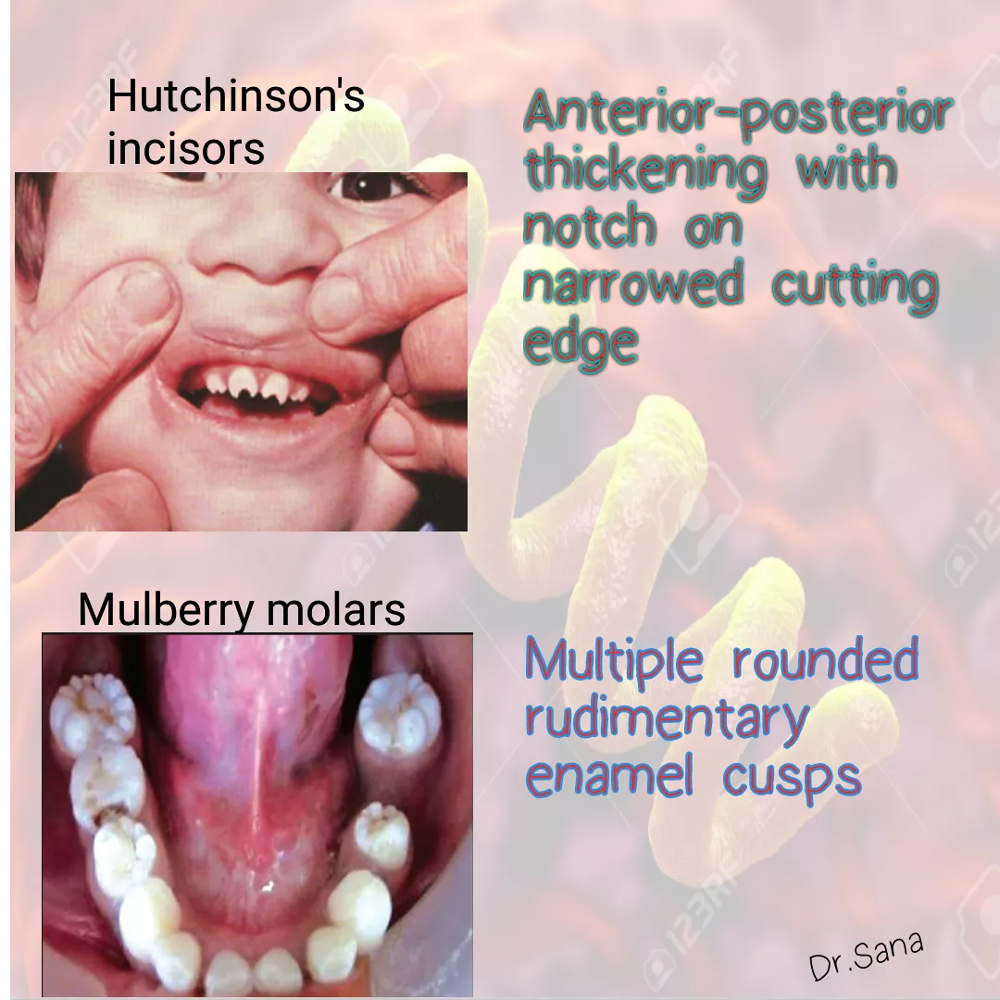
*Congenital syphilis: Due to T. pallidum crossing the placental barrier
Classical appearance: saddle nose, frontal bossing, sensorineural deafness, Hutchinson incisors (peg-shaped with notch), and mulberry (Moon) molars.
Type 1 is the most common viral infection affecting the mouth. Type 2 causes genital infection.
- Primary HSV called primary herpatic gingivotomatitis
- Spread by direct contact.
Clinical picture:
Age: children and infant
Site: attached gingiva, sometimes on the dorsum of the tongue.
Oral manifestation: It presents with a single episode of widespread stomatitis and unstable mucosa with vesicles that break down to form shallow painful ulcers
Systemic manifestation: enlarged, tender cervical lymph nodes, halitosis, coated tongue, fever, and a general malaise for 10–14 days.
Management: bed rest, topical and systemic analgesia, a soft or liquid diet with extra fluid intake, and chlorhexidine mouthwash. Severely ill or immunocompromised patients should receive systemic aciclovir.
Generally self-limiting
- Recurrent infections: The virus remains latent in trigeminal ganglion until activated by trauma, UV light, stress, cold, or Immunosuppression.
Oral manifestation: Prodromal phase (burning/tingling) over 24h is followed by vesiculation and pain.
Management: Lesions may respond to 1% penciclovir or aciclovir 5% cream.

Herpatic gingivostomatitis

Herpis labialis
It neurogenic virus
- Primary infection: Chicken pox
Spead: airborne.
S&S: Classically, an itchy, vesicular, cutaneous, centripetal rash affects children with a peak age of 5–9yrs and rarely affects oral mucosa.
Management: self-limiting, palliative care.
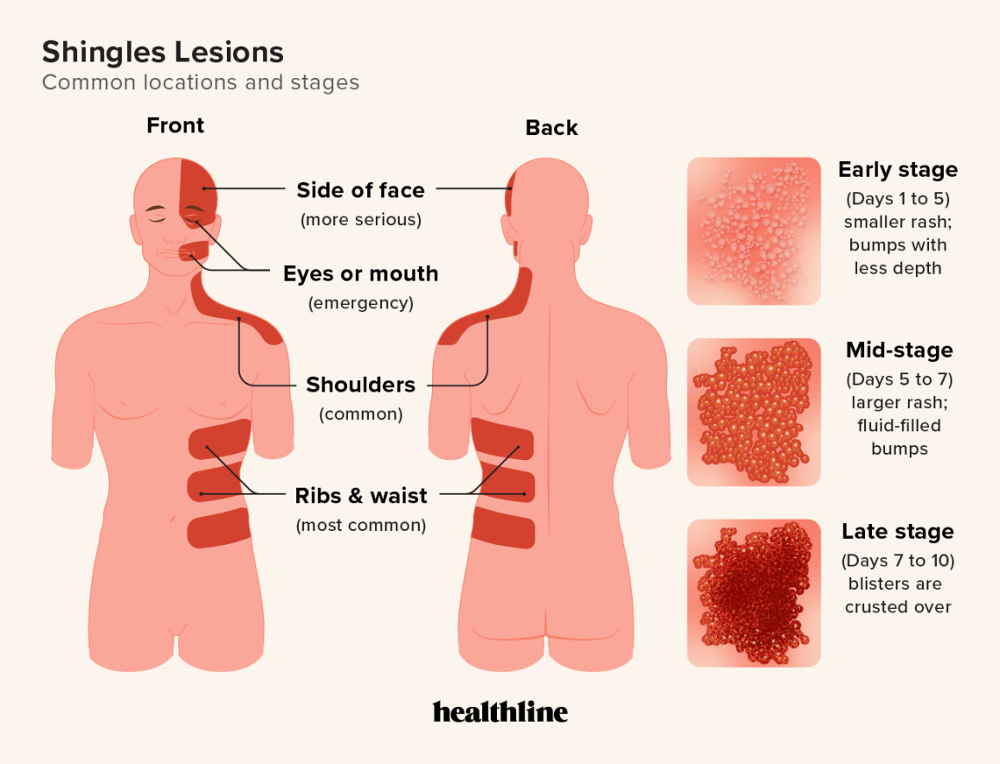
- Recurrent infection: Shingles, the virus remains latent in the Trigeminal ganglion.
S&S: presents as a unilateral lesion, never crossing the midline. Facial or oral lesions may arise in the area supplied by the branches of the trigeminal nerve., pre-eruption pain, followed by development of painful vesicles on skin or oral mucosa, which rupture to give ulcers or crusting skin wounds.
Management: Aggressive early treatment of shingles with aciclovir
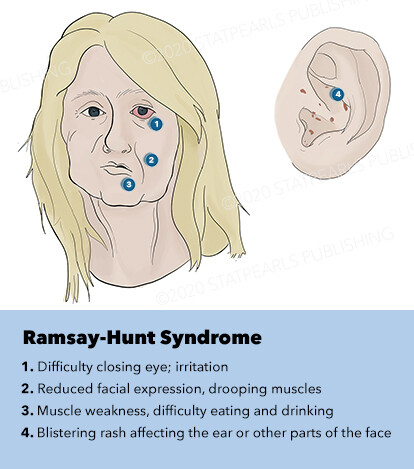
NB: Ramsey-Hunt Syndrome (herpes zoster oticus)
reactivation of the virus in the Geniculate Ganglion affecting CN VII and VIII resulting in facial paralysis, deafness and vertigo, tinnitus, vesicles in the ears on the affected side.
Management: antiviral, damage is permanent after 1 week, prednisone, physiotherapy.

Chicken pox
Causative Agent: Coxsackie virus (A16, 5, 10)
Spread: oro-fecal route.
Symptoms: Oral mucosal vesicles that break down, leaving painful superficial ulcers, particularly on the palate, gingiva is rarely involved, on the skin, and a papular, vesicular rash appears on the hands and feet, nasal congestion is a common accompanying symptom
Treatment: self-limiting, Resolves in 10-14 days
Causative Agent: caused by the Coxsackie A virus.
Spread: oro-fecal route.
Age Group: Primarily affects children.
Symptoms: small oral ulcers in the affecting uvula, palate, and fauces (posterior part of the mouth) with no gingivitis Fever, and general discomfort can be mistaken as teehting.
Treatment: Self-limiting within 10–14 days.
Herpangina
Age Mainly affects children and young adults.
Spread: infected saliva.
General Symptoms: including sore throat, fever, and lymphadenopathy, headache and malaise, and often a maculo-papular rash.
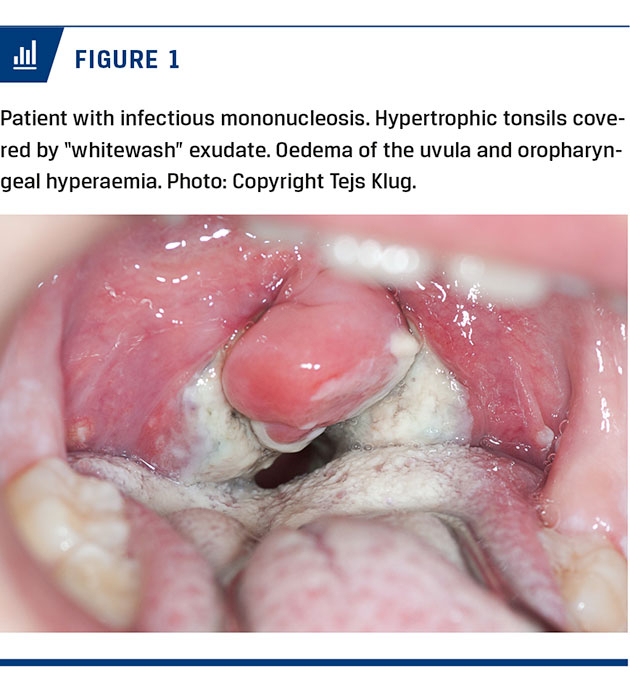
Oral symptoms: mimic 1° herpetic gingivostomatitis, with widespread oral ulceration, and in addition petechial hemorrhages, especially at the junction of the hard and soft palate
Viral Causes: Primarily caused by Epstein–Barr virus (EBV).
Diagnosis: Paul–Bunnell tests
Treatment: Focused on relieving symptoms.
Caution with Antibiotics: Avoid ampicillin to prevent adverse reactions.
Opportunistic infection on the tongue mucosa by EBV is thought to be the pathological mechanism behind ‘hairy leucoplakia’, which is found in transplant and HIV-positive patients.
- C. albicans and C. dubliniensis are by far the most important. It is found in the mouths of >40% of the symptom-free population
- Risk factors: in denture wearers, immunocompromised (including diabetics, steroid users, and HIV-infected patients), smokers, xerostomia, malignancy (radiotherapy/chemotherapy), malnutrition, and broad-spectrum antibiotics.
- Type:
- A-Acute candidosis:
- 1-pseudomembranous candidosis: Thrush:
Site: oral mucosa of the cheeks, palate, oropharynx, tongue.
Symptoms: Creamy plaques on erythematous that can be gently stripped off, leaving a raw under-surface, may be presented as discomfort while eating, a burning sensation, or bad taste.
In infants, may be associated with facial and nappy rash can lead to mutual recolonization between breastfeeding mothers and infants.
Treatment:
- Topical antifungals (nystatin, miconazole) provide limited benefit.
- Systemic antifungals (fluconazole, itraconazole) are highly effective.
- Chlorhexidine mouthwash is a helpful adjunct.
Resistance: require Candida subtyping.
Drug Interactions: Azole antifungals interact with drugs like warfarin and statins.
Diagnosis: Hyphe can be identified under the microscope using PAS and KOH stain.
- 2-Erythematous candidosis:
Cause: Opportunistic infection due to broad-spectrum antibiotics, inhaled steroids, HIV, or xerostomia.
Site: dorsum of the tongue
Symptoms: Painful red, shiny, atrophic oral mucosa; worsens with hot or spicy foods; may co-occur with thrush.
Treatment:
- Address underlying cause (e.g., rinse mouth after using inhaled steroids or use a spacer).
- Treat as for thrush.
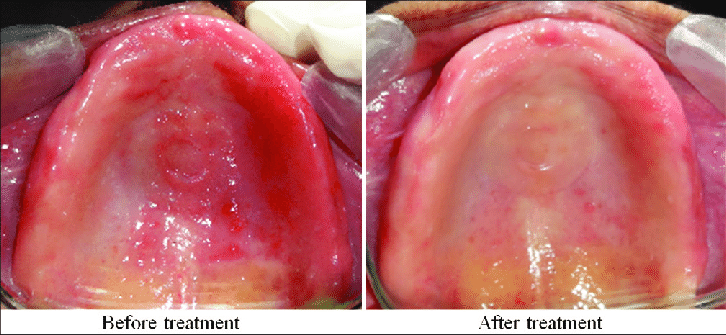
1-Denture stomatitis (chronic atropic canidosis/ denture sore mouth) is typically symptomless and appears as redness, petechiae, and whitish areas under full dentures
Site: the upper palate.
Incidence: Affects 30–60% of full denture wearers, females> males(4:1 ratio).
Causes:
Mainly caused by Caida albicans (90% of cases) and other Candida spp.
Contributing Factors include :
Poor denture hygiene, night-time denture wear, high sugar intake, trauma, systemic factors (e.g., nutrient deficiencies, xerostomia, endocrine disorders).
Management:
- Remove dentures at night
- Maintain good denture hygiene (brushing and soaking).
- Reduce sugar intake.
- Apply miconazole gel to denture fitting surface.
- Replace poorly fitting dentures if necessary.
- Address systemic factors; refer to a general medical practitioner (GMP) if needed.
- Treat coexisting papillary hyperplasia surgically if required.
- Consider systemic fluconazole for severe cases.
2-Angular chelitis: is a combined infection (Staphylococcal, β-haemolytic streptococcal, and candidal)
Site: the angles of the mouth.
Causes:
Local factors: Trauma, inadequate denture vertical dimension.
Systemic factors: Iron deficiency, vitamin B12 deficiency anemia.
Symptoms: Red, cracked, macerated skin at mouth corners, often with a gold crust.
Diagnosis: Investigate full blood count (FBC) and haematinics to identify systemic factors.
Treatment:
Apply miconazole cream for at least 10 days after clinical resolution.
Eliminate underlying factors.
Use mupirocin cream in anterior nares to eradicate Staphylococcus aureus sources.
3-Median rhomboid glossitis:
Site: the dorsum of the tongue,
Risk factor: inhaled steroid use and smoking.
Symptoms: occur on the center of the tongue and palate ("kissing lesions").
Treatment: Treat only if symptomatic; topical antifungals can alleviate discomfort but will not improve appearance.
Address underlying causes, excluding haematinic deficiencies and diabetes
4-Candidial leukoplakia (chronic hyperplastic candidosis):
Symptoms: white patch, that can to be scrapped of nor distinguished from leukoplakia, commonly affecting middle-aged male smokers,
Site: bilaterally on oral commissure the buccal mucosa or dorsum of the tongue.
Risk: Increased risk of malignant transformation.
Diagnosis: Confirm through microbiological and histopathological analysis.
Treatment:
Systemic antifungals (e.g., fluconazole, itraconazole).
Address underlying deficiencies (iron, folate, vitamin B12).
Encourage smoking cessation.
Reassess if lesions persist; consider surgical excision if dysplasia is present.

Erythematous candidosis

Median rhomboid glossitis:

Angular chelitis

Candidial leukoplakia
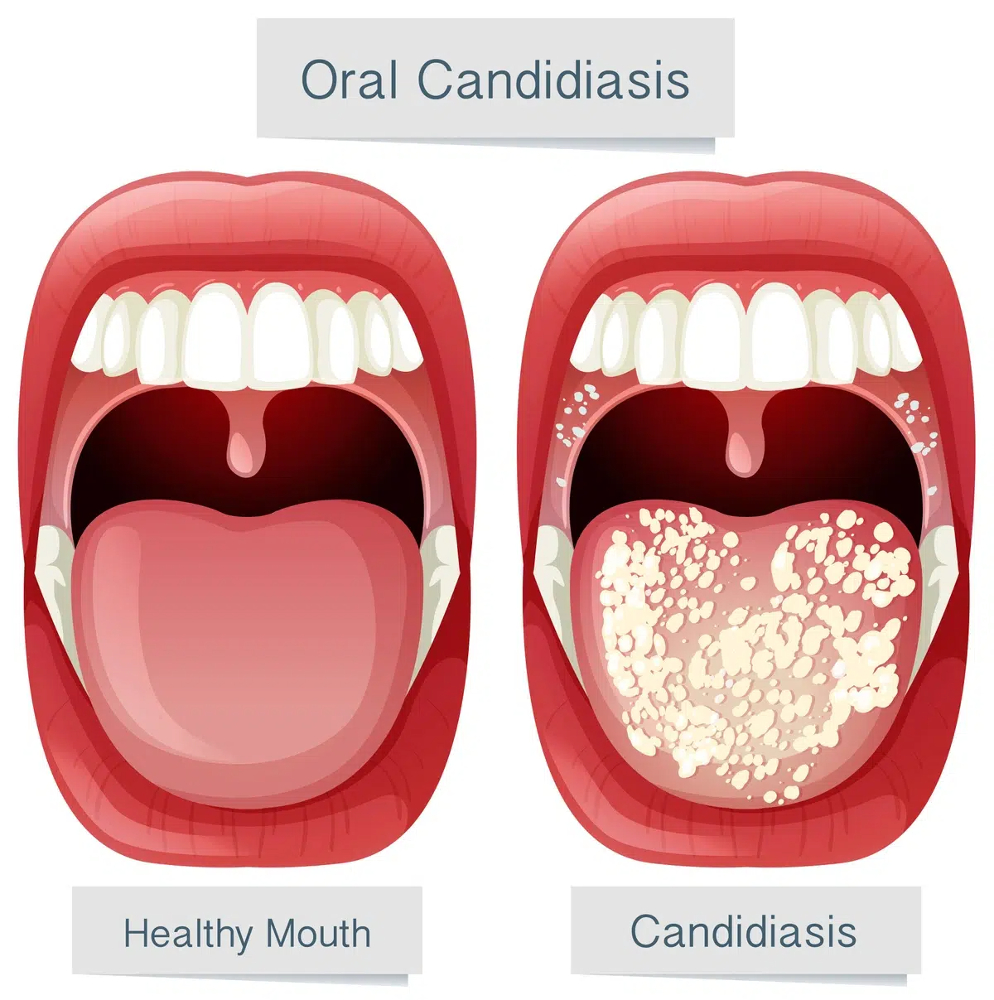
oral thrush
denture stomatitis
These are characterized by recurrent oral ulceration.
Triggers: Stress, trauma, menstruation, toothpaste (sodium lauryl sulfate), drugs (NSAIDs, alendronic acid, nicorandil), smoking, allergies, and deficiencies (iron, B12, folate).
Associated Conditions: Crohn’s disease, ulcerative colitis, gluten enteropathy.
- There are three subgroups:
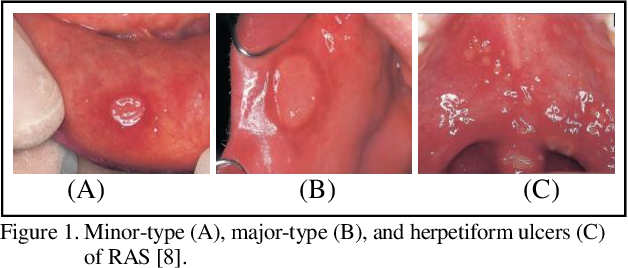
- Minor:
Prevalence: Very common 80% (RAS) cases.
Demographics: Begin in childhood or adolescence; 45% have a familial history.
Features:
clinical: Appear as 1–6 ulcers, 2–5 mm in diameter, Prodromal discomfort often precedes the ulcers
site:non-keratinized mucosa.
Cause: Likely a T-cell-mediated immune reaction in genetically predisposed individuals (HLA A1, A11, B12, DR2).
Treatment: Heal within 1–2 weeks without scarring and recur every 1–4 months.
- Chlorhexidine mouthwash.
- Relieve pain using analgesics or benzydamine mouthrinse.
- Topical steroids (e.g., hydrocortisone 1%) or tetracycline (e.g., oxytetracycline 3%).
- treat underlying deficiencies or conditions (FBC, haematinics, etc.).
Prevalence: Seen in 10% of RAS cases.
Features:
Clinical: Larger ulcers (>10 mm), causing tissue destruction, scarring.
Site: any site in the mouth and oropharynx
NB: associated with gastrointestinal/haematological disorders and AIDS.
Treatment: Same as minor aphthae but may include topical/systemic steroids.
Prevalence: Least common, more frequent in older females.
Features:
Clinical: Resemble primary herpetic stomatitis and appear as a crop of up to 100 small, painful ulcers
Site: floor of the mouth, lateral margins, and tongue tip (keratinized and non-keratinized mucosa).
- Heal in 1–2 weeks, rarely merge into large ulcers with scarring, and recur frequently for 2–3 years.
- Treatment: Same as minor aphthous ulcers.
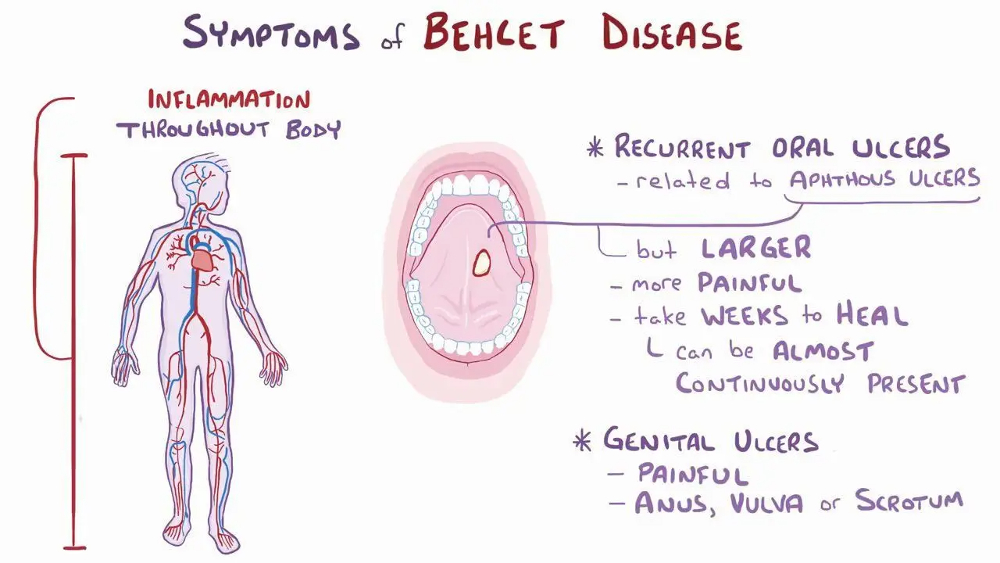
severe relapsing and remitting systemic vasculitis, primarily affecting venules, with the potential to affect all organs.
Prevalence: Common in the Far East, Silk Route ,More severe in males and typically seen in young adults.
Symptoms:
Clinical: resembles RAS, recurrent oral ulcers (often the first sign of autoimmune disease), recurrent genital ulcers, eye lesions (e.g., uveitis), or skin lesions (e.g., erythema nodosum, folliculitis).
- Skin hyper-reactivity, raised ESR, and IgA levels.
Diagnosis: According to International Study Group (ISG) criteria, at least two of the major features (oral, genital, ocular lesions) must be present, excluding other
Pathergy test: erthymatous nodules after 24-48 hours of needle prick.
clinical causes.
Treatment:
Ophthalmic referral if eye involvement is present.
Monoclonal anti-TNF for severe mouth ulcers.
Management includes local and systemic corticosteroids, often alongside immunosuppressants.
Complications: blindness, can be fatal in cases with vascular involvement (e.g., aneurysm rupture, thrombosis).
Role of Dentists: Dentists play a critical role in early detection of autoimmune diseases like Behçet's syndrome.
- Intraepithelial bullae: are caused by loss of attachment between individual cells (acantholysis).
1) Pemphigus is a chronic autoimmune skin disease that can be fatal without treatment (mortality 10%).
Types: P.vegetans less common, Pemphigus vulgaris is the most common type, affecting the oral mucosa in 95% of patients, often as the initial presentation.
Aetiology: Autoimmune condition with circulating autoantibodies (IgG) targeting epithelial desmosome tonofilaments (desmoglein-1(skin) and desmoglein-3 (oral), causing acantholysis (separation of the epidermis) and fluid-filled bullae that rupture, leaving easily infected ulcers., causing acantholysis (separation of the epidermis) and fluid-filled bullae that rupture, leaving easily infected ulcers.
Incidence: in middle-aged (F > M), particularly in Jews and Arabs. Rarely, it may be drug-induced or paraneoplastic.
Clinical: the first identifiable lesions are quite often found in the mouth. These are usually seen as ulcers because the bullae break down rapidly
Site on the palate
Differential Diagnosis: Can be confused with conditions like aphthae, lichen planus, candidiasis, and pemphigoid.
Diagnosis:
Nikolsky sign: Stroking the mucosa induces a bulla.
Histology and Immunofluorescence: Direct or indirect immunofluorescent tests using fresh biopsy samples. presence of TZANK cells: degenerated epithelital cells.
Treatment:
Systemic steroids and/or immunosuppressive agents (e.g., azathioprine, dapsone, mycophenolate mofetil, gold, cyclophosphamide for refractory cases).
Biologic agents (e.g., rituximab) and calcineurin inhibitors are promising newer treatments
NB:
Benign familial chronic pemphigus (Hailey–Hailey disease) This differs from other pemphigus by having a strong family history, with onset of the disease in young adults.
2)viral infections: *^
3) Epydermolysis bullosa:
is a group of inherited bullous conditions, with Simplex most common form. Other variants are subepithelial.
Inheritance: autosomal dominant or recessive inheritance pattern.
Symptoms: Skin blisters form due to mild trauma, leading to scarring and disfigurement (no growth of fingernails, constricted oral orifice, hypoplastic teeth, failure of teeth eruption.
Simplex Type: Caused by mutations in the K5 or K14 gene, disrupting basal cells and causing bullae formation.
Management: .Treatment is symptomatic and preventive, with extra care needed to avoid oral lesions during dental treatment.
- Subepithelial bullae: separate the epithelium from the underlying corium.
1) Angina bullosa hemorrhagic
an acute, localized oral blood blister of unknown cause,
Causes: trauma may lead to a break in the epithelium-connective tissue junction, causing bleeding from superficial capillaries
Clinical: red purple bulla develops during eating and can be alarming to the patient.
Prevalence: Most common in the elderly, and steroid inhalers
Sites: Soft palate, cheeks, and tongue
Diagnosis: Exclude other bullous conditions, especially pemphigus and pemphigoid.
Treatment: The main approach is puncturing the blister and providing reassurance.

Angina bullosa hemorrhagic
2)Mucous membrane pemphigoid
a chronic autoimmune condition,
Prevelance: most common in females over 60 years old.
Symptoms: Bullae are blood-filled and tense, often associated with desquamative gingivitis. The conjunctiva may be affected, leading to vision loss if scarring occurs. Symblepharon:scarring of the canthus of the eye.
Natural History: The disease alternates between periods of activity and inactivity, sometimes remaining quiescent for years.
Diagnosis: Histology and direct/indirect immunofluorescence reveal antibodies (mainly IgG and C3) at the basement membrane level against Laminin-332
Management: topical steroids and systemic steroids (with or without azathioprine, methotrexate, or dapsone).
Ophthalmology referral is important to prevent ocular damage.
3)Bullous pemphigoid:
- Age: over 60 years old.
- Clinical: It involves subepithelial bullae that are firm, and less likely to break down compared to those in pemphigus.
Oral mucosa is affected in about 20% of cases.
Can be associated with internal malignancy or drug-related immune response.
Cause: autoantibodies (IgG) targeting the epithelial basement membrane (BP 180)
4) Dermatitis Herpetiformis: A rare chronic condition often linked to gluten sensitivity.
cause: Autoantibodies target reticulin, gliadin, endomysium, and transglutaminase. Clinical: Oral lesions occur in 70% of patients with skin lesions. bullae in the mouth break down, leaving large erosions. vesicles on the shoulders, back, buttocks, elbow which are extremely pruritus.
Age:middle-aged men.
Treatment includes dapsone (both diagnostic and therapeutic) and a gluten-free diet.
5)Epidermolysis Bullosa: A rare skin disease with various forms.
dystrophic autosomal recessive:
Clinical:
Oral manifestations soon after birth, causing bullae formation from minor trauma.
-These bullae break down, leaving painful erosions. The dentine may be affected, leading to hypoplasia and a high susceptibility to caries.
-Healing involves scarring, which can make eating, speaking, and swallowing difficult. Skin involvement: extremity destruction and potentially carcinomatous changes
6)Erythema Multiforme:
An immunologically mediated hypersensitivity reaction that affects the skin and mucous membranes,
prevelnce: commonly seen in young adult males.
Trigger agents include drugs (e.g., carbamazepine, penicillins, NSAIDs), infections (e.g., HSV, mycoplasma pneumonia), pregnancy, malignancy, and chemicals (e.g., perfumes, food additives) that leads to immune complex depositing in superficial BV causing vasculitis.
Clincical:
-Oral lesions affect 70% of cases. oral mucosa is covered in bullae which break down, the lips and gingivae becoming crusted with painful erosions.
Site: affect anterior mouth (on the lips and gingiva).
Skin lesions ‘target lesions’, concentric rings of erythema on the palms, legs, face, or neck.
Minor forms self-limiting in 3–4 weeks, but recurrence can happen once or twice a year.
Severe forms include Stevens-Johnson syndrome and toxic epidermal necrolysis: oral mucosal lesions, preceded by flu-like symptoms, and involvement of the genitals eyes, and pharynx.
Management:
withdrawing or treating the trigger,
supportive therapy, and antiviral treatment if related to herpes.
Severe cases may require steroids and azathioprine, while mild cases can be managed with topical steroids.
7) Linear IgA Disease:
autoimmune disease.
Produces non-specific oral ulceration and rarely bullae. causes dense blisters.
treatment: Systemic steroids or mycophenolate mofetil.